Innovations
Anne-Marie Riedinger was awarded her MA in Medical Illustration in 1982. She pursued her studies at Illinois University, Chicago and introduced comfortable, soft silicone prostheses into France in 1985. Her prostheses are totally life-like due to the painstaking integration of all the colour nuances in the pre-baking phase. They can also be attached directly to the skin with adhesive and adopt facial expressions. These state-of-the art prostheses took over from the hard, uncomfortable, surface-painted resin prostheses available at that time and latex prostheses that were fixed onto spectacle frames.
The first revolution: bone implants
Her meeting with the team led by Professor P-I Brånemark, inventor of titanium implants, was a defining moment. She rapidly extended the application of bone-anchored implants to facial prostheses. Fixation to the bone combined with the suppleness of the silicones heralded a true revolution in anaplastology. Adhesives and frames were done away with, and the prostheses were now soundly held in place via implants by being clipped onto gold bars or more recently using magnets.

A-M Riedinger and prof. Brånemark
Anne-Marie Riedinger made the very first bone-anchored prostheses in France in 1986 for the Necker Hospital for Sick Children in Paris, in collaboration with Dr Hamann and Prof Manach.
Furthermore, Prof P-I Brânemark is also the inventor of the bone-anchored hearing aid, BAHA, which is often associated with an auricular prosthesis for our patients.

Photos 1 and 2: the hearing aid is placed behind

the retention system for the outer ear prosthesis.

Photo 3: After the prosthesis has been put in place on the magnet counterparts.
The use of implants combined with soft silicones results in a firmly attached prosthesis enabling a broad spectrum of patients and more complex cases to be treated.
Our surgical collaboration has continued with the aim of constantly improving prosthesis retention, dealing with the peripheral area around cavities, improving the ease with which prostheses can be set into position, including for children and people with reduced dexterity, and simple hygienic care. Surgeons are happy to place implants on patients who have undergone radiotherapy, thereby continuously pushing back the limits of what we can do. Moreover, our prostheses are removable, can protect an open cavity, enable the site to be monitored and sometimes remain the only option available for facial reconstruction.

Second revolution: the arrival of 3-D
In the first decade of this century, state-of-the-art technology revolutionised the world with 3-D tools. Surface scanners and 3-D printers began to find their niche on the market. However, at that time this very expensive technology was reserved for a few rare institutions.
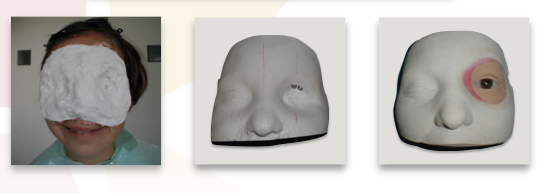
At the Centre during this period, taking facial impressions was arduous for our patients, especially when they had open cavities. Moreover, in order to blend the orbital prosthesis into the face, a broad impression was required and the patient had to keep their eyes closed for a long time. In all cases, modelling requires great technicity and proven artistic qualities.
However, from 2010 onwards, 3-D printers and surface scanners gradually became more affordable. At this time, the Centre d’Épithèses Faciales was collaborating in research projects and thanks to subsidies from the Regional Authorities and the Public Investment Bank, we were able to integrate 3-D for certain phases of prosthetic fabrication from 2013 onwards. Complex printouts could be made without touching the patient, who were able to keep their eyes open. Once more, the boundaries of feasibility were pushed back ever further.

(1) Scanner 3D
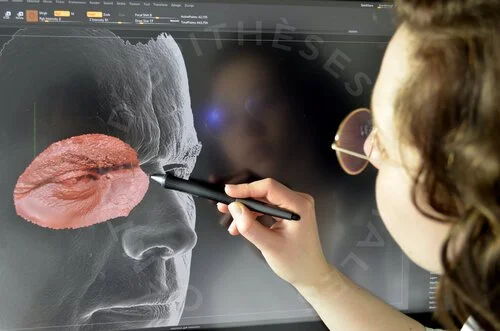
(2) 3D Software

(3) 3D Print
We use a surface scanner (1) and printout out patients’ faces with a 3-D printer. Some prostheses are designed virtually using 3-D software, which allows us to make a mirror-image copy of the ear or the region surrounding the ear (2). We then print out the face and the ear or the eye (3) on our 3-D printers. A wax copy of the prosthesis template is then positioned before making final adjustments on the patient.
Traditional methods are nonetheless still in use when making the mould and applying the silicone colours inside the mould. These essential phases are carried out in our Centre thanks to our artistic and technical expertise.
Furthermore, we also establish surgical guides if necessary in order to optimise the position of attachments as part of our collaboration with the surgical team.
In conclusion, the Centre d’Épithèses Faciales has developed 35 years of know-how with talented anaplastologists, setting up unique protocols for the bespoke colouring of our silicones and creating optimum combinations according to the characteristics desired, which are specific to each patient. Moreover, we have gradually improved the retention systems thanks to our 35-year-long experience in surgical collaboration and we have optimised the ease with which prostheses can be put in place and hygienically cared for.